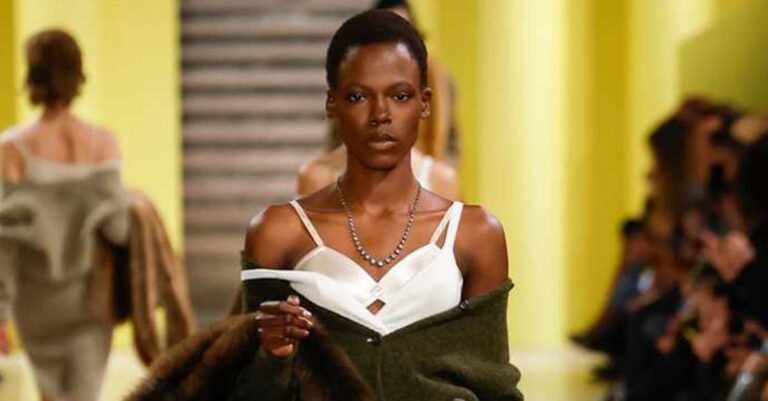
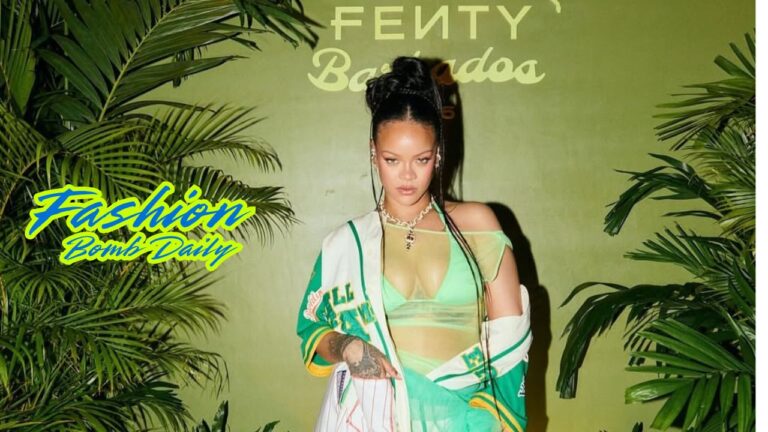
News Arts & Entertainment John Mulaney Jokes About Olivia Munn Having 'Cancer Brain' March 13, 2025 Automotive Montclare Automotive Corp: Delivering Trusted Auto Repair Services to Chicago Drivers January 23, 2025 Books & Literature The Wheel of Time Sets Up the Dominos in “Seeds of Shadow” March 13, 2025 Building & Construction How DOGE will impact Washington, DC-area apartment owners March 13, 2025 Business Accurate Air Solutions: Elevating HVAC/R Services in Lubbock, Texas March 11, 2025 Cryptocurrency Ethereum Testnets Holesky Reaches Finality Following Pectra Upgrade Launch March 13, 2025 Education The Intersection Of Psychology And Technology: Enhancing Human Well-Being In The Digital Age March 13, 2025 Family & Parenting The Most Surprising Accessory at Paris Fashion Week? Bras March 13, 2025 Fashion & Beauty Rihanna Celebrated the Latest Fenty X Puma Collection in a White Pinstripe Jersey and a Seafoam Green Skirt March 13, 2025 Finance The stock market is wobbly. Is now a good time to change how much I invest? March 13, 2025 Foreign Language Bijouterie Hidous : Luxe intemporel et bijoux personnalisés au cœur de Montréal March 2, 2025 Gov & Politics RFK Jr. Suggests Getting Measles Is Better Than Getting Vaccinated March 13, 2025 Health & Fitness What The Far Side taught me about belonging in science March 13, 2025 Home & Garden 12 Great Sofas For Small Spaces March 12, 2025 Lifestyle The Art of Doing Nothing: How to Create Your Own Personal Retreat Day March 13, 2025 Real Estate Gateway Realty of North Platte Celebrates Over 50 Years of Trust and Excellence in Real Estate October 23, 2024 Religion From the Ashes of the Palisades and Eaton Fires, Treasured Mementos Restore Hope January 29, 2025 Science Trump's EPA takes steps to roll back dozens of environmental regulations March 12, 2025 Sports No post found! Technology NASA set to bring astronauts home after 8-day mission turns into nine months March 12, 2025 Travel The 2025 Air Canada eUpgrade Strategy March 12, 2025
Montclare Automotive Corp: Delivering Trusted Auto Repair Services to Chicago Drivers January 23, 2025
The Intersection Of Psychology And Technology: Enhancing Human Well-Being In The Digital Age March 13, 2025
Rihanna Celebrated the Latest Fenty X Puma Collection in a White Pinstripe Jersey and a Seafoam Green Skirt March 13, 2025
Gateway Realty of North Platte Celebrates Over 50 Years of Trust and Excellence in Real Estate October 23, 2024