Karen, age 46, mother of two, is a world-renowned physician who has headed numerous clinical trials and has saved many lives. She suffered from public speaking anxiety disorder. Mike, age 26, a college graduate, spends most of his life in his room. He doesn’t work, is socially paralyzed, and spends over 100 hours a week with various technology dependencies. His parents walk on “eggshells” for fear of triggering his anger. This has resulted in long-term enabling of what has become an addiction to avoidance.
While these two cases personify opposite ends of the functioning spectrum for social anxiety, both have dynamics in common. These are anxiety based on performance dynamics, dissociation, and a clinical cocktail of PTSD and OCPD. Karen’s perfectionism drove her public speaking anxiety in formal presentations. Mike’s perfectionism manifested in his selective mutism, where he believed he had to have the perfect thing to say in any interactive scenario. For example, he did have two gym buddies, but he wouldn’t go to the gym if they were not there. He described his primary fear: “someone may want to work their way onto the machine and might start a conversation with me.” He was frozen by his selective mutism.
Both Karen and Mike had trauma in their reservoir. The reservoir is one’s conscious and unconscious past and present. Karen’s trauma was a combination of excessive internal critical script training for perfectionism—something she referred to as “Palo Alto syndrome”—and unresolved emotional content related to an aggressive male. For over 25 years, she had dissociated from these. Mike’s trauma included a combination of peer rejection, developmental struggles with OCD, a void of paternal nurturing, and overcompensatory maternal attempts at nurturing.
What they do not have in common is initiative for their mental health. Karen was lecturing around the world and was confused as to why her performance panic seemed to appear out of nowhere. She was highly motivated to fix the problem. Mike was agitated and overwhelmed upon any attempt to move out of his primitive lifestyle and limited comfort zone. “Initiative” for healing was a foreign concept as he was paralyzed by shame and embarrassment. He remained stuck based on his belief that he “was born this way and nothing could be done about it.” His parents’ conflict with each other and “egg shell” anxiety resulted in a long-term, deeply ingrained “compulsion to avoid.”
In a nutshell, what is social anxiety?
Having well over 50,000 clinical hours under my belt since 1978, I’ll first tell you what it’s not. It’s not simply generalized anxiety with the word “social” thrown in front of it. This approach of lumping anxiety orders together all too often characterizes mental health marketing, which sets the consumer and practitioner up for unrealistic expectations.
Anxiety disorder of the millennium
According to a November 1991 article in the Journal of Clinical Psychiatry, “social phobia is an emerging problem that is just beginning to receive attention and will be taking the limelight among anxiety disorders. What separates social anxiety from other anxiety disorders is that it is based on performance.”
That’s over 30 years ago. Major advances in technology have enabled interactive avoidance. Many studies, including an article by Dwight Silverman of The Houston Chronicle, show that “texting has replaced talking as the most common form of communication.” This may not mean much to a millennial or Gen Z, but it’s startling to me. It is symptomatic of an epidemic of verbal communication avoidance and social skills deficits.
In addition, COVID-19 has been a tremendous enabler of avoidance.
The ICD-10 F40.10 defines social anxiety as an “anxiety disorder characterized by an intense, irrational fear of one or more social or performance situations in which the individual believes that he or she will be scrutinized by others. Exposure to social situations immediately provokes an anxiety response. In adults, social phobia is recognized as excessive or unreasonable.”
The Diagnostic and Statistical Manual of the American Psychiatric Association (DSM-5) 300.23 currently defines social anxiety disorder as “a persistent fear of one or more social or performance situations in which the person is exposed to unfamiliar people or to possible scrutiny by others.”
Clinical reality is there are subsets on a wide range of functioning levels. While there are many manifestations of the disorder, there are two basic types: individuals with and without initiative.
I define social anxiety as an emotional and cognitive attack on personhood associated with autonomic hypersensitivity overload. Social anxiety goes to the core of self-esteem. The core dynamic of the pathology is the inability to differentiate performance from personhood.
Social anxiety is the classic disease of resistance, as most sufferers will do anything to avoid introspection and interoception. Introspection is the examination of one’s mental and emotional processes. Interoception is our seventh sense. It’s the ability to be aware of internal sensations in the body, such as heart rate, respiration, temperature, pain, and more. It’s a collection of senses that can be conscious or subconscious.
Resolving social anxiety is about channeling psychophysiological energy. This energy is an internal phenomenon.
Emotere
In “3 Ways to Better Understand Your Emotion” (Harvard Business Review 11/10/16), Susan David writes, “dealing effectively with emotions is a key leadership skill. Naming our emotions is an important first step in dealing with them effectively. But it’s harder than it sounds; many of us struggle to identify exactly what we are feeling, and often the most obvious label isn’t the most accurate. This is a process of approaching one’s inner experiences in a mindful way rather than trying to suppress them.”
Let’s take this a step further. The Latin word for emotion, “emotere,” is defined as “energy in motion.” Individuals who suffer from social anxiety are, in general, detached from this internal energy. One of my patients, a 40-year-old scientist with performance anxiety and concurrent dysthymia, had the initiative to rate on a 1-10 scale the intensity of her specific emotions in her journaling.
Karen’s case is an example of specific performance anxiety. Mike is an example of pervasive social phobia. When anxiety morphs into avoidance, it becomes a phobia. Both cases are examples of social anxiety.
I received a call from the mother of a 26-year-old who was suffering from pervasive social phobia. She said, “I would like you to see my son.” I said, “I need to see the parents first.” She responded with indignation, “why do you want to see us? He’s 26 years old.” I responded, “why are you making the call?” The avoidance-dependence dynamic is a complex dynamic that holds psychotherapists hostage. Think about it! The over-18-year-old is primitively functioning, socially avoidant, and overly dependent with no initiative for mental health. In most cases, this person will want to have nothing to do with therapy. In the case where the over-18-year-old is in therapy, the usual pattern is that parents are not involved. This is due to a variety of reasons, including: (1) the 18-year-old will not want it, (2) the therapist will not know how to facilitate parenting and family engagement, and (3) the parents want nothing to do with treatment and have the attitude that the therapist should fix the adult child!
This is a confusing subject. For example, Susan had her first and only date at age thirty-eight. She maintained a low-level civil service job. Her only socialization was in a weekly special needs group. During her appearance with me on Oprah in 1988, Oprah said, “I don’t understand. Were your parents so much fun you wanted to hang out with them all the time?”
There is something drastically wrong with this formula. This is the reason a case like this must be positioned as a “family challenge.” Treatment needs to be initiated by the caregivers who need to learn an empowering, non-enabling strategy. Thinking otherwise will be a poor investment, as the pathology of avoidance will accrue.
Gold standard for treatment = trivializing the disorder
A number of research articles, including Nayeefa Chowdhury and Ahsan Khandoker’s “The Gold Standard Treatment for Social Anxiety Disorder: A Roadmap for the Future” in Frontiers in Psychology, describes the behavior therapy-exposure therapy with extinction model as the “gold standard for social anxiety treatment.” As does “Why Cognitive Behavioral Therapy is the Gold Standard of Psychotherapy for Social Anxiety Treatment” by Daniel David, Ioana Cristea, and Stefan Hofmann in Frontiers in Psychiatry (Jan 2018).
All too often, the behavior therapies promise “gold standard results” in a short-term treatment framework for social anxiety. In my opinion, this marketing does not meet integrity standards. The research trivializes the disorder. In fact, many of my patients who have done well in treatment have said, “it’s the hardest thing I’ve done in my life.”
A comprehensive article, “Researching the Research on Cognitive Behavioral Therapy,” is available at www.socialanxiety.com Tip of the Month Club (January 31, 2020).
The bottom line is everything starts with a thought (conscious or not), which leads to behavior. Negotiating this dynamic is what CBT is all about, which makes a lot of sense. That said, leaving out the emotion-physiology connection will have limited treatment results. My therapeutic formula includes four domains. Think of FATE.
F = function (physiology)
A = action (behavior)
T = cognition (thinking)
E = emotion (emotere)
Statistics are helpful to understand prevalence, but in the case of social anxiety, they aren’t completely adequate to define the condition, which has attained epidemic proportions. It’s not a subject most sufferers are open to discussing because of shame and embarrassment. People with avoidant personalities are experts at avoiding. Perfectionists don’t want to admit non-perfection. My high-functioning achievers, like Karen, with public speaking anxiety, will wait for the last possible moment to get help—when their careers are threatened, often after decades of struggle. Patients with a profile like Mike only enter treatment if facilitated by caregivers.
The Anxiety and Depression Association of America estimates that 15 million adults have social anxiety. This number swells when you consider stats, such as the Chapman University Survey of American Fears (2019), which found that 10.7 percent of Americans have a public speaking phobia, and 21.2 percent to 23.3 percent fear public speaking. Similarly, a 2001 Gallup poll found that 40 percent of adults in the United States fear public speaking.
Consider the following additional statistics for social anxiety-related symptomatology:
- Selective mutism, defined as a compulsive inability to speak in specific situations. Selective mutism affects almost 0.47 percent to 0.76 percent of children.
- Hyperhidrosis, or excessive sweating, which can lead to phobic avoidance due to fear of being noticeably nervous, affects 2.8 percent of Americans.
- Erythrophobia, or blushing anxiety, affects 5 percent to 7 percent of Americans.
- Avoidant personality disorder, a condition that occurs in 2.1 percent to 2.6 percent of people.
In addition, when considering special needs populations, the statistics grow due to a multiplicity of processing challenges.
A complex clinical profile
There is extensive comorbidity associated with social anxiety. This includes substance and technology over-dependence, depression, and a variety of personality disorders. These commonly include avoidant, dependent, OCD, OCPD, and narcissism. These can morph into a complex clinical profile, which often falls between the cracks of clinical profiling.
I first discovered social anxiety in 1978 while working as a youth worker in a community center on the North Shore of Long Island. At the suggestion of a colleague who worked with the Girl Scouts, we started a socialization group for teens with learning disabilities. After doing intake interviews, many of the participants never showed up for the group. Welcome to social anxiety!
Technique vs. core work
To really understand social anxiety, it’s important to understand dissociation. Dissociation is detaching from the mental processes of thoughts and emotions. It manifests in many forms. It is a defense mechanism. One’s defensive positioning can be a compulsion. Social anxiety sufferers become very skilled at dissociating because they do not want to experience the “pain of emotere.” The result of the detachment is that repressed emotional energy morphs into the physical symptoms of anxiety and other comorbidities.
Kelly, age 32, lived independently in a parent-funded condo. She worked at the counter at a local bakery. She socialized two times a year with co-workers. She never dated. Her favorite activity was watching re-runs of The Golden Girls. She dissociated by playing old radio songs in her head as she compulsively paced back and forth for hours as her primary evening activity.
David, age 49, has eight children. He is very successful in commercial real estate. He is a community organizer. He is a philanthropist. He studies Talmud 20 hours per week. He is always too busy for introspection as he is compulsively engaged in creating external processes.
Todd, age 45, had played semi-professional baseball and worked in commercial real estate. He was an imposing figure at 6’6 “. He had been struggling with public speaking anxiety for many years. At our first session, he said to me, “your book (Work Makes Me Nervous) was great, but don’t insult me by saying something about my past is related to anxiety.” He was all in for technique but obviously resistant to core work. We were not compatible.
Understanding the content in one’s reservoir is a necessary foundation for healing because that’s where the unresolved “emotere” is.
Tension myositis syndrome
Approximately twenty years ago, I worked with Cindy, who was a would-be singer and disco queen at age 45. Her role model was Madonna. She suffered from stage fright before every performance. In addition, training was a challenge because of over-dependence on alcohol and cannabis. I knew of a physician, the late John Sarno, M.D., who treated back pain. I suggested she read his book, Healing Back Pain: The Mind Body Connection. She skipped the book and went directly for an appointment. In the next appointment with me, she shared his study guide. Connecting to Sarno’s work was a milestone in my clinical journey.
To dumb it down, Sarno’s work is based on the dynamic that repressed emotion is so powerful it inhibits the flow of oxygen, creating a condition he called tension myositis syndrome. The primary repressed emotions are rage, emotional pain, sadness, fear, and feelings of unworthiness in the unconscious mind. In essence, any physical symptom that does not have a biological etiology to it is a symptom of TMS. Social anxiety is very much a manifestation of TMS.
The brilliance of Sarno’s work is how he organizes the content in one’s reservoir. The domains of the reservoir include (1) childhood, (2) self-imposed pressures based on personality traits, (3) the pressures of life, and (4) other emotions.
A full reservoir means the brain must produce symptoms to protect from these feelings. This causes the physical symptoms of anxiety.
In the reservoir is trauma. There are three types of traumas: acute, chronic, and complex. An example of obvious trauma is Alana, age 34, who worked as an administrator in commercial shipping. She grew up in Ukraine. Both parents were alcoholics. Her father abused her mother physically and mentally. Her father abused her mentally and often forced her to buy vodka for him when he was comatose. Alana was responsible for getting them both into rehab to no avail. Her father’s friend tried to rape her. She grew up in a state of constant hypervigilance.
A much less obvious example of trauma is Tim, age 25. He grew up in a wealthy real estate family, which was loving and supportive. He could do no wrong. He was the “golden child.” Expectations were quite high. Over time, the pressure to be perfect accrued. It drove his internal critical script into toxic territory with unrealistic expectations regarding perfection. This was his trauma.
An example of acute trauma for Alana was when, at age 16, her father’s friend drove her into the woods and tried to rape her. An acute scenario for Tim was when he learned that he did not make the varsity baseball team in college after being a star in high school.
More insidious than acute trauma is the chronic, ongoing nature of toxic influences and the complex way they impact self-esteem!
Experiencing a first panic attack is trauma. The post-panic ongoing struggle, where obsessive rumination dominates, becomes chronic and complex.
“When the trauma is resolved, there are no more triggers.”
This statement by Dan Siegel during a training seminar on interpersonal neurobiology really hit the mark. Crucial for healing is the core work of identifying target memories in one’s reservoir where the following were learned:
- Negative association to adrenaline
- Hypervigilance
- Over-adaptation to fear of judgment
- How personhood vs. performance became at risk.
Attaching to this reservoir energy is foundational work for the clinical objective of self-regulation. It is based on bringing emotere to a conscious level and crossing the bridge from the intellectual mind to the emotional.
For example, Sean, age 50, a salesman, “was not convinced” about reservoir relevance in his initial stage of treatment. In a breakthrough moment of introspection and interoception, he was able to identify the same adrenaline-energy he experienced when he and his siblings were lined up waiting for mom to use her belt for corporal punishment as the same energy he experiences anticipating speaking in public.
PTSD merges with OCPD = the perfect storm
When the trauma in one’s reservoir merges with the perfectionism of obsessive-compulsive personality disorder, the result is the perfect formula for performance anxiety.
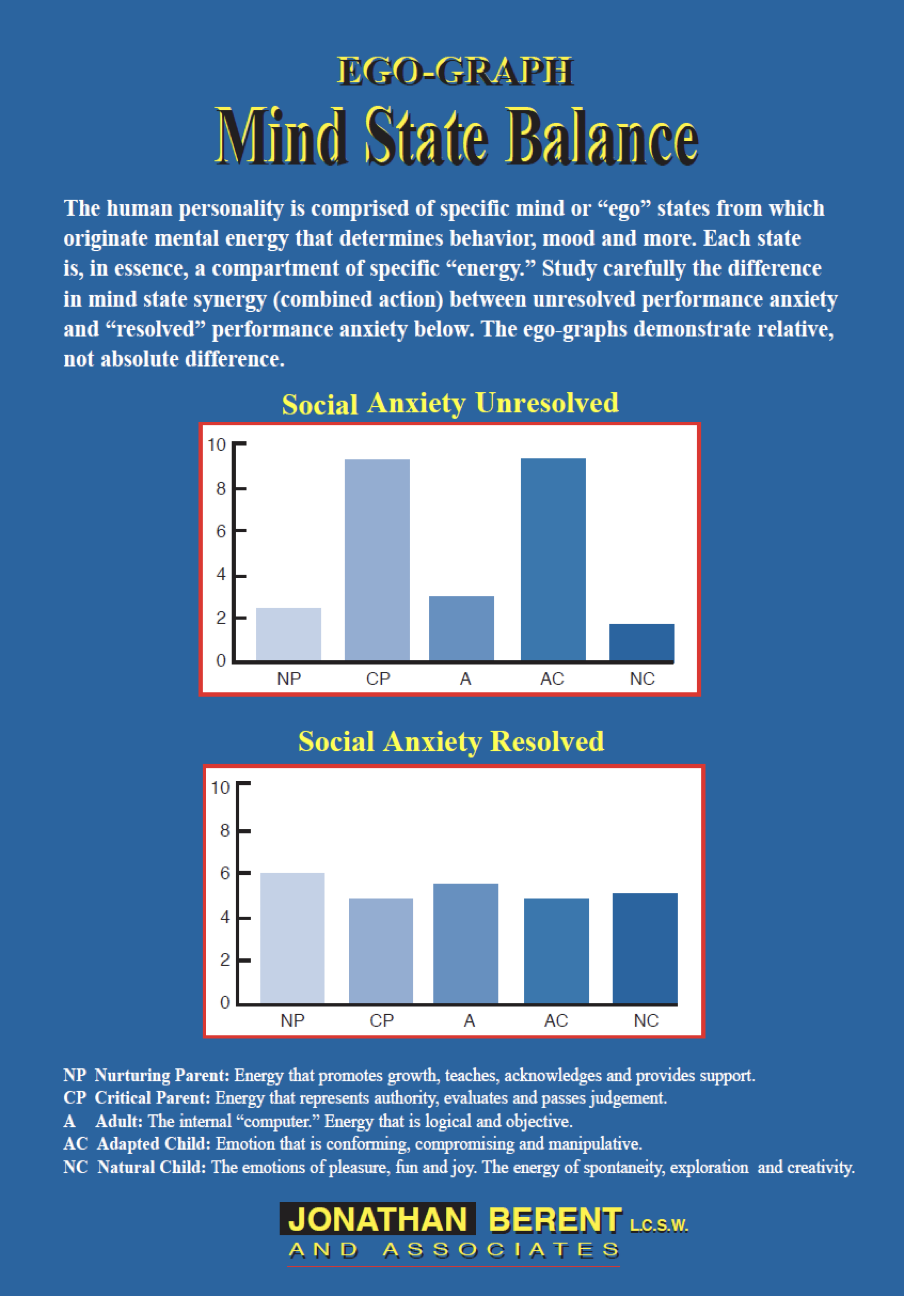
The following ego-graph is based on the psychology of transactional analysis developed by Eric Berne and others in the 1960s. The concept of the ego-graph was developed by John M. Dusay. In mind-state terms, it provides a visual of what baseline pathology and eventual resolution looks like. All mind states are important. There is no such thing as a bad mind state. The issue is synergy and balance.
The “twin towers” of the critical parent and adapted child mind states provide a visual of unresolved trauma.
The towers represent a deeply ingrained “mind tic.” This is not a neurological tic but a deeply ingrained psychophysiological reflex between the toxic critical script and the over-adaptive self.
As the excessive critical parent activates excessive adaptation, the mind tic is created. As the adapted child learns to be hyper-vigilant about perceived threats, pressure on one’s nervous system accrues over time. The critical parent-adapted child interaction becomes a reflex that is ingrained and automatic.
The formula for anxiety resolution and high performance is to nurture the natural child with a good dose of adult. The “resolved” ego-graph represents the objective of treatment.
While technique is certainly important, core work that includes introspection and interoception is critical for true healing and what I reference as “a high-performance mind,” which means developing a proactive approach for health and happiness. Both technique and core work need to be integrated for high-performance treatment.
Journaling, surfing, and response prevention as a technique
Building on Sarno’s methodology, I integrated journaling into my work about twenty years ago. During this time, no patient has reached a quality state of therapeutic productivity without it. Journaling is the key technique for introspection and interoception. That said, this has been a difficult “cross-fit” process for many of my patients. Those who have embraced it have experienced a substantial boost in their learning curve.
“Surfing” is the primary technique for adrenaline control. There are four steps:
Realistic expectations: This means that “fight or flight” adrenaline will be present (in different degrees) in challenge scenarios. Do not waste any time hoping it will not be. This is a huge concept. If the critical script puts unrealistic expectations on the inner child, like there should not be any energy present, the result will be strain and more adrenaline.
Acceptance: This is the hardest. This means going with the adrenaline instead of fighting it or trying to suppress it. Do this with the interpretation that it is your friend and source of energy.
Go with the wave: The surfer goes with the wave and harnesses its energy.
Take one or two diaphragmatic breaths: The breath is the most valuable tool available to control nervous system energy.
Many social anxiety sufferers are challenged with OCD and OCPD symptoms. Therefore, exposure and response prevention encourage facing fears and letting obsessive thoughts occur without putting them right or neutralizing them with compulsions. To organize this technique, as well as surfing, it is important to create a hierarchy of anxiety at the beginning of treatment so that the patient can take on this challenge in a methodical manner.
Basic thoughts on medicine
When I started my practice in 1978 utilizing biofeedback and counseling to treat stress-related disorders, a primary objective was to help without pharmacology. Forty-five years later, I’ve discovered that there are significantly empowering ways to integrate psychopharmacology into the treatment process. Lowering the mind tic on the ego-graph is the primary objective of medicine for social anxiety. Decreasing these mind states creates neuroplasticity and more potential to nurture the natural child with a good dose of adult. In cases where medicine is indicated, I encourage the patient to think of it as a metaphorical pregnancy; meaning to utilize it for nine months or longer, the goal of which is to wean off the medicine after therapeutic goals are achieved and sustained. That said, this can be complicated as many patients enter treatment having been on medicine long-term and have no clue of any proactive therapeutic strategy. In addition, many patients who have positive results with the medicine do not want to stop taking it.
Oprah and Sally
In 1988, shortly after I appeared on The Oprah Winfrey Show, I was on the phone with the producer of The Sally Raphael Show. The first thing he said was, “You were on Oprah; we don’t want you.” Then he asked, “Why do you have a public relations firm?” My response: “I want to educate the world.” The result was a wonderfully produced show that generated a few thousand phone calls. There was no internet. The bottom line is that the world still needs to be educated.
Jonathan Berent is a psychotherapist.